Sept. 14, 2023

For 40 years, researchers have unsuccessfully tried to explain — or debunk — the “Hispanic Paradox,” the finding that Hispanic Americans live several years longer than white Americans on average, despite having far less income and health care and higher rates of diabetes and obesity. Now, armed with more comprehensive data, powerful genomic tools, and a rich cultural awareness of the communities they study, a new generation of scientists is finally making headway.
These researchers, many Hispanic themselves, are boring down on the paradox, trying to understand which parts hold up, which don’t, and how it’s evolving as immigration patterns shift. They are also looking at what the survival edge can teach us about further improving the health of Hispanics, who make up nearly one-fifth of the U.S. population, and improving health for the rest of the country as well.
They’re finding that for Hispanics, living longer does not necessarily mean living healthier, and that lumping together people from places as varied as Brazil, Mexico, and Puerto Rico conceals important health risks for these individual populations, which may as a result go unnoticed by many American physicians. They’re also finding that healthy Hispanics who immigrate to the U.S. tend to get sicker the longer they stay — raising deeper questions about why our wealthy nation, which spends more than $4 trillion on health care, is far sicker than it should be.
“Part of the story about the Hispanic Paradox,” said Kyriakos S. Markides, a professor of aging at the University of Texas Medical Branch in Galveston, “is that the non-Hispanic white population is not doing as well as it should.”
Markides coined the term “Hispanic Epidemiological Paradox” in a 1986 paper showing Hispanics in the American Southwest lived as long, or longer, than white people. The finding was met with widespread disbelief and criticism. Markides, a junior faculty member at the University of Texas Health Science Center in San Antonio at the time, said colleagues warned him against publishing the finding because they thought it was so obviously wrong.
“Everyone said the data is bad,” Markides recalled in an interview with STAT. “But I kind of stuck my neck out with a colleague and published.” Over time, as more Hispanic people were included in epidemiological studies, new data confirmed his findings. But researchers kept looking for reasons to overturn the paradox.
First, there was “the salmon bias,” which said many Hispanic immigrants weren’t included in U.S. mortality numbers because they return to their native countries to die. An analysis of Social Security data showed the salmon bias was too small to explain the paradox.
Then there was “the healthy migrant effect,” the idea that those able to emigrate voluntarily were unusually fit. That does seem to be true, but doesn’t fully explain the life expectancy gap, according to a detailed analysis conducted this year by a group of three Hispanic economists. They also debunked the idea that Hispanic deaths are fewer because the population is younger: When data are adjusted for age, the paradox still holds.
Other ideas, such as the role of diet — along with culturally insensitive paper titles such as “A review of the Hispanic paradox: time to spill the beans?” — have come and gone. While it’s true that legumes might fend off disease-causing inflammation, there hasn’t been conclusive evidence that food explains the longevity, and the diets of many immigrants worsen quickly after they reach the U.S.
Another explanation — that death certificates used in the original research were imprecise because Hispanic people were often erroneously classified as white — has been cast aside; the findings have held as the demographics of death reporting have become more precise.
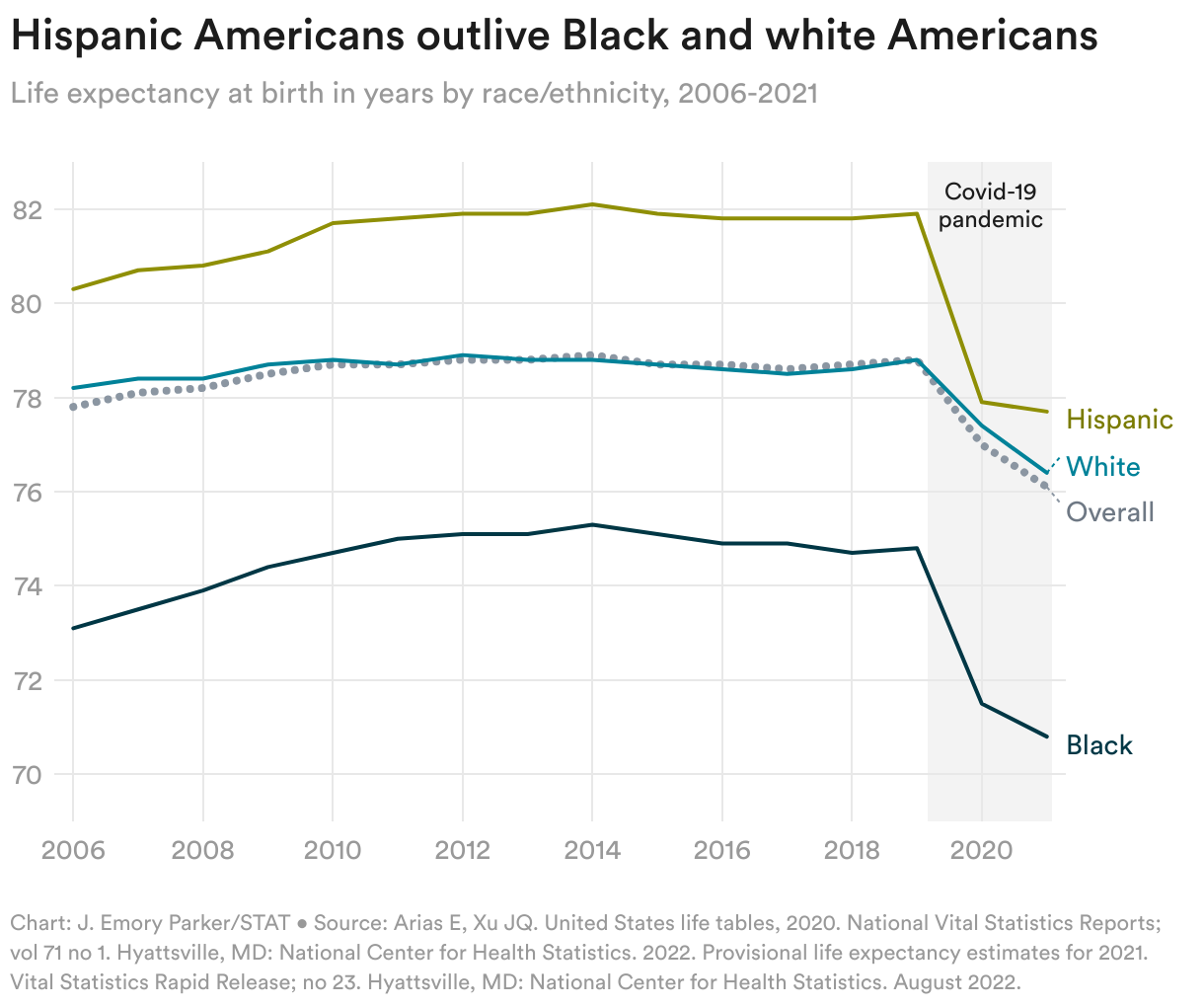
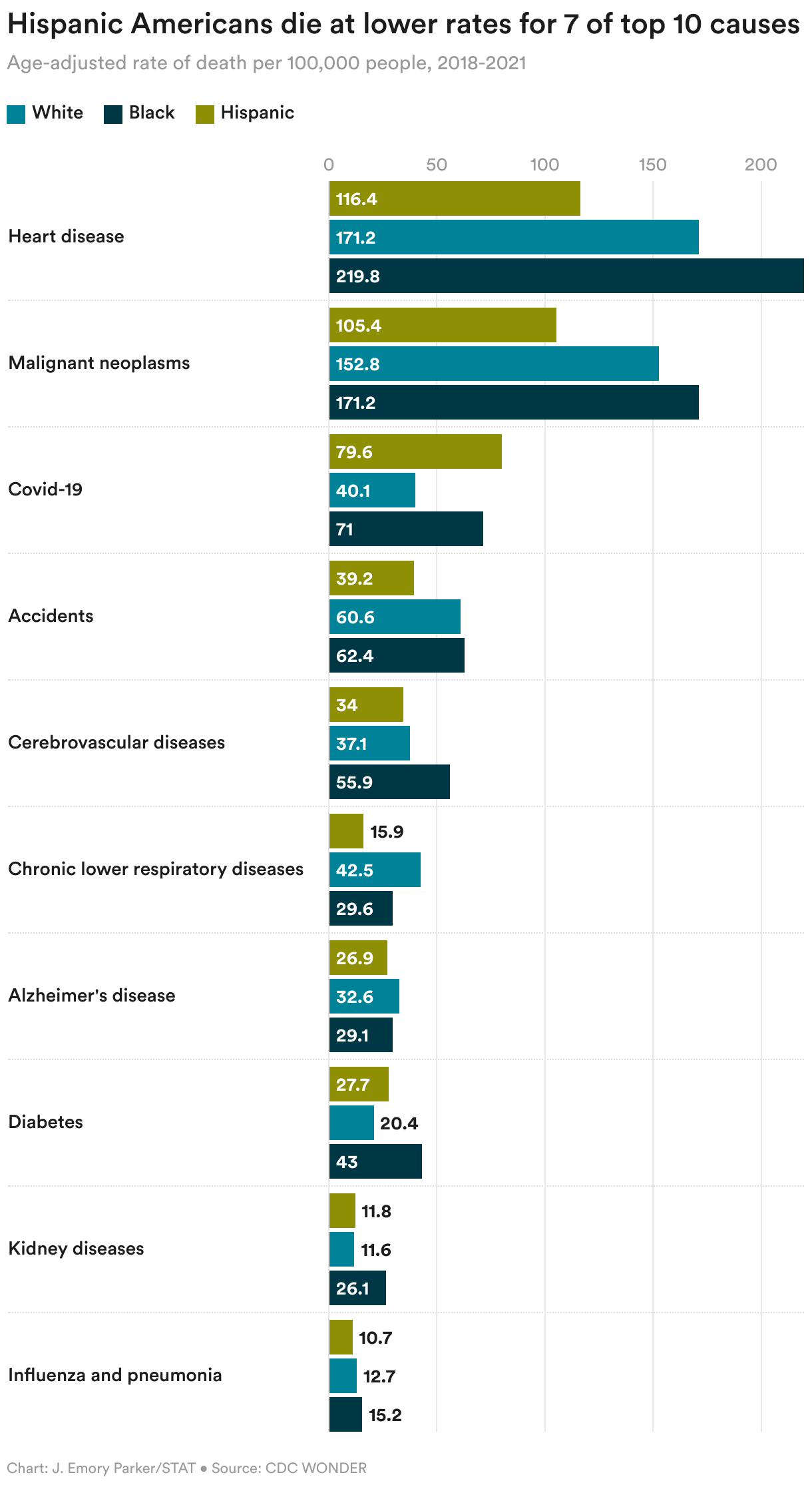
The turning point for Markides came in 2010 when the National Center for Health Statistics released a report showing Hispanic Americans had a life expectancy more than two years longer than white Americans. A few years later, the Centers for Disease Control and Prevention weighed in with a lengthy report stating that mortality data for 2013 showed Hispanic Americans had lower death rates for most leading causes of death compared to white people. “The findings in this report are consistent with previous reports that use the term ‘Hispanic Paradox,’” it stated.
“It’s real,” said Markides, who continues to study the underpinnings of the paradox and whose original paper has now been cited by other researchers more than 1,500 times. “We can argue about how big it is, but it is sizable.”

John Ruiz was in high school in California’s Simi Valley when the original paper by Markides and Jeannine Coreil first appeared. He first came across it as a young researcher in the early 2000s when he tried, and failed (due to a dearth of data on Hispanic health at that time), to locate one simple statistic: the average blood pressure for a Hispanic male. He vowed to turn his attention to the paradox once he had tenure and more freedom to research issues he cared about.
In 2012, then an assistant professor at the University of North Texas, he did so, publishing a meta-analysis of 58 studies confirming the paradox did exist and showing that U.S. Hispanic populations had a 17.5% lower risk of mortality from any cause compared to other racial and ethnic groups. “It might be time to move beyond the question of the existence of the Hispanic mortality paradox and onto investigations into the causes of such resilience,” he wrote at the time.
A decade later, he’s still waiting. More researchers, he argued, need to study what it is that Hispanics may be doing right. “There’s a very entrenched idea that non-Hispanic white health is the gold standard and all minorities have disparities,” he said. “People tend to point out role models, people who do well. There’s no reason we can’t do that at a population level and try to understand why Latinos are doing well.”
Ruiz, now a professor of clinical health psychology at the University of Arizona, is doing just that, focusing on the tight-knit family and community networks that exist among many Hispanics and how they might improve health outcomes for a variety of diseases.
Nascent research in the area gives hints at what might be at play. One study suggested foreign-born Hispanic women with better birth outcomes than those in other groups had more “tenacity, agency and spirituality” that might underlie their resilience. Other research on what’s been termed the “Barrio Effect” shows people in high-density Hispanic neighborhoods have better health outcomes, despite sometimes higher levels of crime and poverty.
A variety of factors — from having someone home to help you if you fall or to remind you of a medical appointment, to living in a large group that together can manage unexpected bills — could contribute to better health, Ruiz said.
The movie “Coco,” a 2017 Disney animated film exploring strong Mexican familial ties even after death, “is a beautiful example of that social network and the importance of family bonds across the life span and beyond,” he added. “Frankly, one is never alone.”
Other researchers note that America’s two longest-living racial and ethnic groups — Asians and Hispanics — both live in collective cultures. “That’s a lesson. That’s an intervention that can be done,” said Ruiz, who is working to assess resilience to cardiovascular disease and late-stage lung cancer in Hispanic populations.
More recently, some have declared the end of the paradox because of the Covid-19 pandemic, which killed Hispanic people at high rates. But data for 2021 show Hispanics were still outliving white people by more than one year.
And a paper published in 2020, Ruiz noted, showed the paradox was global and not tied solely to immigration; in addition to Hispanics living in the U.S., people living in countries such as Nicaragua, Colombia, Cuba, and Peru lived longer than whites in the U.S., possibly due to lower smoking rates and more cohesive social and family networks.
“It expanded the paradox to say not only is this happening in the U.S., it’s happening globally as well, even in countries far poorer,” Ruiz said. “Now we’re not only talking about one paradox but several.”
Even as the paradox has gained acceptance, another recent paper delivered a different and more important message: Hispanics may live longer, but they tend to live sicker. And they may carry a disease burden that lasts for decades.
The research showed that Hispanic men in the U.S. had rates of heart disease higher than those in both white men and, in what was a surprise to many, Black men. And Hispanic women had more heart disease than white women.
The Puerto Rican physician who led the study first learned about the paradox when he was in medical school in the late 1980s and has been inspired by and been teaching others about it ever since. “Obviously being Latino, I’ve always been interested in this. I’ve always believed in it,” said Olveen Carrasquillo, an assistant dean and professor of medicine and public health at the University of Miami Miller School of Medicine.
Carrasquillo’s study involved data from All of Us, the National Institutes of Health program building a database that better reflects the nation’s genetic diversity. Carrasquillo thought he’d play with the data available so far, a cohort of more than 40,000 Hispanic participants, to test things he knew were true, like the paradox. But when he analyzed the genetic data along with electronic health records, he found the opposite of what he expected: high rates of cardiovascular disease among Hispanics.
“We didn’t believe it,” he said. “We went back and checked with other statisticians.” The result held.
Carrasquillo is the first to say he hasn’t overturned the paradox. “It’s one study,” he said. And his data were on disease rates, not mortality rates that are the cornerstone data of the paradox. “It just adds to the puzzle,” he said.
In the meantime, he said, it’s clear Hispanic people need to control their diabetes, obesity, and blood pressure. “Even if my study had shown the paradox,” he said. “I would still argue we need to do a better job at taking care of Latinos.”
Markides couldn’t agree more. For decades he’s been running a longitudinal study of nearly 4,000 older Mexican Americans, seeing their health erode as they age, acculturate, and suffer the impact of lives often filled with hard physical labor, discrimination, and little quality medical care. “They are more disabled, subject to chronic diseases like diabetes, and also cognitively impaired,” he said. “They do need help. They need medical care.”
“I always say, ‘Hispanics, we live long and suffer,’” said Jane Delgado, a Cuban American who serves as president and chief executive officer of the National Alliance for Hispanic Health. Delgado argued in a recent New England Journal of Medicine editorial that the way the Hispanic Paradox has been handled by researchers — with data ignored because findings did not fit prevailing notions and cultural biases — has been a missed opportunity to rethink how we all view health and prevention.

It’s not surprising Hispanic health was little studied until recent decades. It wasn’t until 1980 that the U.S. Census added a question about ethnicity. And early health research focused almost exclusively on Mexican Americans because they long made up the bulk of Hispanic immigration. But that’s now changing.
As more data become available, some researchers are separating out health outcomes for Hispanics who are Puerto Rican, or are of Cuban or Mexican descent. For Luisa Borrell, that’s not enough.
Borrell is a distinguished professor of epidemiology and biostatistics at the Graduate School of Public Health and Health Policy at the City University of New York and an associate editor of the American Journal of Public Health. She’s also Dominican — one group of Hispanics, along with Salvadorans, for which there are almost no health studies, despite the fact that both groups make up a growing share of the U.S. Hispanic population as immigration from Mexico declines.
In 2008, Borrell was one of the first to analyze hypertension in Hispanic groups other than Mexican Americans. She found that Mexican Americans were indeed less likely to report having hypertension than white Americans, as were Central and South Americans — as the Hispanic Paradox would predict. But she found something that had been missed: Dominican Americans reported even more hypertension than Black Americans.
“These findings call for data disaggregation beyond the standard racial/ethnic categories,” she wrote at the time.
To Borrell’s frustration, few large national studies separate Hispanic participants into subgroups. (The NIH’s Hispanic Community Health Study is one notable exception.) Not doing so is easier, she noted, and gives researchers the bigger sample sizes they want, but it can be misleading, as she has found in paper after paper.
When she looked at mortality rates for Hispanic women in 2012, she found they differed by Hispanic subgroup, but also by whether the women were U.S.- or foreign-born. In a 2022 study looking at birth outcomes for Hispanics in New York City, she found that Mexican American and South American infants did fare well for their birthweight, as the paradox suggests. But the same was not true for Cuban infants. She also found infant mortality was higher for Puerto Rican and Dominican infants, compared with those who were white.
“We cannot keep lumping all Hispanic people together,” said Borrell. “Hispanic people are coming from 27 countries at least.”
Borrell said the focus should not be on proving or disproving the Hispanic Paradox, but rather understanding it — especially as it, and immigration patterns, evolve. She fully expects the paradox to shrink, and maybe even disappear altogether, as Mexican Americans with their life expectancy advantages become a smaller share of the new immigrant population and as immigrants already in the U.S. continue to age and adopt the unhealthy ways — higher rates of smoking and drinking and eating processed food — of their new country.
Esteban González Burchard has been obsessed with ancestry ever since he was a child and wondered why his Mexican American mother was so much darker than him. He used to ask, as he snuggled up to listen to her read: “Are you really my mother?” Studying genetic ancestry has since become the cornerstone of his dogged, decades-long research career; he thinks it will go a long way to understanding the Hispanic Paradox.
Burchard had graduated from Stanford Medical School and was training at Harvard in the early 1990s when his advisers, all noted researchers, came to him with a conundrum. Mexican Americans are known to have some of the lowest rates of asthma in the U.S., but new CDC data showed Hispanics in the Northeast had much higher rates of the disease. The senior researchers couldn’t figure out what was going on.
It took Burchard — “a Mexican kid born in California that studies genetics,” as he describes himself — about five minutes to figure it out: The Hispanic population in the northeastern U.S. wasn’t primarily Mexican American, like it was on the West Coast. It was Puerto Rican.
Meanwhile, another incident from medical school had stayed with him. A Black teenager had died from an asthma attack just blocks from the Harvard teaching hospitals, clutching an inhaler. Burchard started to put things together: He surmised higher rates of asthma in some Hispanic groups, rivaling those in Black Americans, was tied to ancestry. It’s known that Puerto Ricans have a higher percentage of African ancestry than Mexican Americans.
But it would take decades more for Burchard, who now runs the Asthma Collaboratory at the University of California, San Francisco, to sort through the complex genetics of asthma and find proof. There was little genetic research done on Hispanics when Burchard started out: Participants in the Framingham Heart Study were largely white, the company deCODE genetics famously analyzed an Icelandic population for its important early database, and many national genetic biobanks contained overwhelmingly white participants. “In the U.S., no one was studying non-whites,” Burchard told STAT.
Wanting to change that, Burchard helped start the Genetics of Asthma in Latino Americans study at Brigham and Women’s Hospital in Boston, and later brought it to UCSF. Because not enough subjects were being recruited at U.S. sites, Burchard helped open research centers in Puerto Rico and Mexico City, as well as in Hispanic neighborhoods in San Francisco.
Over the years, his group has linked increased African ancestry in some Hispanic groups to higher rates of asthma susceptibility and severity — answering that question about high asthma rates in some populations he’d encountered so long ago. His lab has also used whole genome sequencing to understand why albuterol inhalers — the most commonly used drug to treat asthma — don’t work for many Puerto Rican and Black children. He thinks increased use of ancestry data and genetic sequencing to tailor treatment choices may revolutionize the care of many diseases, as it has with cancer.
(Along the way, he also found the answer to his childhood questions. Genetic ancestry testing showed that his mother’s ancestry was more than half Native American and less than 40% European while his was 65% European and about 25% Native American.)
Burchard has worked to continue to find genes that play a role in asthma. But he’s found it challenging: NIH reviewers have been less likely to fund, and journal editors have been less likely to publish, genetic work on Hispanic populations — because their rich mixture of Indigenous, Black, and European ancestry, something which no doubt plays a role in the Hispanic Paradox, is seen as too complex and confounding to study.
“All over the world, people used the racial mixture of non-whites to say it was impossible to study genetics in them,” he said. Burchard sees it the other way around: The rich genetic admixture is an opportunity to disentangle the social, environmental, and genetic underpinnings that contribute to varied health outcomes — and result in the paradoxical findings among Hispanic groups.
Burchard is well-aware that his being bilingual — and Mexican American — has aided his important research collaborations with community leaders and physicians in Spanish-speaking countries. As Burchard sees it, if we’re going to understand the paradox, and other health issues facing Hispanics, it’s important to diversify not only the people being studied, but also the people doing the studying.




Exciting news! STAT has moved its comment section to our subscriber-only app, STAT+ Connect. Subscribe to STAT+ today to join the conversation or join us on Twitter, Facebook, LinkedIn, and Threads. Let's stay connected!
To submit a correction request, please visit our Contact Us page.